
General
ACL injury

A cruciate ligament injury is one of the most common issues in sports and recreational activities. This is due to the high stress placed on the knee joint coupled with its extensive range of motion.
Because of this high incidence, the topic is extensively discussed and researched within the scientific community.
In the last "Sport Switzerland" survey conducted by the Sport and Physical Activity Observatory (Federal Office of Sport FOSPO) in 2014, which aimed to paint a detailed picture of the current sporting activities of the Swiss population, 35.4% of respondents stated that they ski [1]. Along with hiking (44.3%), cycling (38.3%), and swimming (35.8%), skiing is one of the most popular sports among Swiss residents [1].
Compared to hiking, however, the risk of injuring the knee and cruciate ligaments, especially the anterior cruciate ligament (ACL), is significantly higher when skiing. Data from the last survey by the Swiss Council for Accident Prevention (bfu.ch) showed that an average of 22,260 people are injured per year while hiking, whereas skiing accounts for approximately 51,700 injuries [2] – 30.9% of these injuries affect the knee joint [3], especially the anterior cruciate ligament. At BodyLab, Osteopathy & Physiotherapy, Rehabilitation and Training in Zurich, we see this reality firsthand every winter season.
Outside of the ski season, football (soccer) is one of the most widespread hobby sports in the world, and Switzerland is no exception. In this sport as well, injuries to the lower extremity occur repeatedly, especially to the knee, as proven by various studies [4].
Various studies estimate that up to approximately 17.6% of football-related injuries presenting to emergency departments involve the knee [5,6,7,8,9].
The majority of these football injuries resulted from non-contact mechanisms (85% of injuries, without the involvement of an opponent), although contact injuries during tackles are of course also possible [10,11].
Anatomy and Function of the ACL
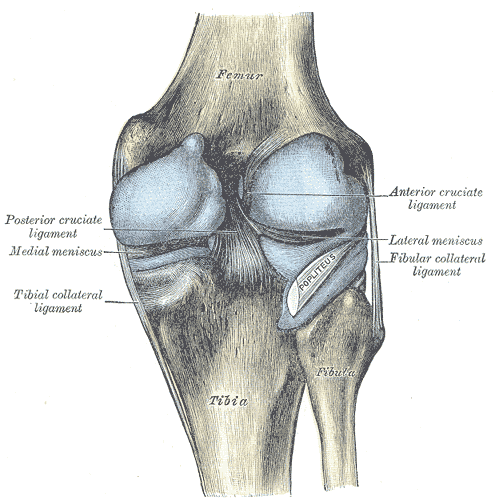
The ACL is one of the most important ligament structures around and inside the knee joint. Together with the posterior cruciate ligament (PCL) and the collateral ligaments, it contributes to the stabilization of the knee joint by stretching from the posterior end of the femur to the anterior part of the tibial head.
The dense connective tissue of the ACL consists mainly of type I collagen fibers and is divided by type III fibers into two primary bundles with different functions. The anteromedial bundle is, on average, 36mm long and comes under tension starting from 30° of knee flexion. Its primary role is to stabilize against anterior tibial translation, meaning it prevents the shinbone (tibia) from sliding forward.
The posterolateral bundle is approximately 18mm long and comes under tension at less than 30° of flexion. This portion of the ACL, together with other ligament structures, serves to stabilize rotational forces in the knee joint.
The ACL is more than just a passive stabilizing structure in the knee joint. Through Vater-Pacinian and Ruffini corpuscles, as well as other free nerve endings in the ligament's insertion area, vibrations, stretching, and shearing forces are perceived. This information is crucial for joint position sense (proprioception) to generate appropriate muscular responses. In the case of the ACL, this triggers increased activation of the hamstrings to reduce anterior tibial translation.
Mechanisms of Injury
A cruciate ligament injury can be triggered by both contact and non-contact mechanisms.
The classic and most common way to suffer an anterior cruciate ligament injury is through a combination of twisting and buckling of the knee joint under load (a forceful valgus collapse of the knee (inward) during slight flexion combined with external rotation).
Injury Mechanisms in Football
Because cleats grip and fix the foot firmly to the turf, immense uncontrolled forces can act on the knee. As a result, 85% of all cruciate ligament injuries in football occur in non-contact situations [10,11]. Video analyses of professional football players also show an increased risk of ACL injury through non-contact situations within the first 9 minutes of the match, as well as a higher risk during defensive and tackling activities [12,13,14].
Injury Mechanisms in Skiing
By means of video analysis of elite alpine skiers after an ACL rupture, Bere et al. identified three distinct accident mechanisms [15]:
Slip-Catch
Dynamic Snowplow
Landing after jumps
Slip-Catch
In almost 50% of all cases, a so-called slip-catch mechanism was the cause. Here, the skier loses snow contact with the outer ski during a turn. Upon regaining snow contact, the ski abruptly catches, resulting in sharp knee flexion, internal rotation of the tibia, and inward buckling of the knee (valgus position). This mechanism often carries with it an injury to the medial meniscus and the medial collateral ligament – known as the Unhappy Triad.
Dynamic Snowplow
Another event (15%) was the dynamic snowplow. Here, the skier is thrown out of balance while leaning back, causing the unweighted leg to drift away and forcing the skier into a split position. The ski rolls from the outer edge to the inner edge, catches in the snow, and forces the knee once again into a valgus position and tibial internal rotation.
Landing After Jumps
The final mechanism (20%) occurred when landing after jumps. The skier loses balance, pushing their body weight backward. In the effort to regain balance, a combination of high knee compression and a major anterior tibia shift (forward movement of the tibia relative to the femur) subjects the ACL to intense stress.
Bearing in mind that professional skiers deal with much greater forces due to their speeds and high-performance equipment, these mechanisms cannot be fully mapped onto the recreational athlete. However, the individual movement factors (deep flexion, valgus alignment, and tibial internal rotation) remain identical.
For recreational athletes, so-called forward twisting falls represent the most common accident mechanism at 54% [16]. This results in a valgus position and tibial internal rotation after catching a ski edge during a turn.
The second most common event is called a backward twisting fall or phantom foot [6]. This rupture mechanism occurs in 26% of all cases. Here, the center of gravity is shifted backward and downward over one leg due to the dropping of the pelvis (increased knee flexion) – whether during a turn or after a fall – and the weight presses on the tail of the ski. Combined with stiff boots, the tibia is forced forward, and the ACL ruptures.
Knee trauma frequently results in concurrent injuries (see Unhappy Triad, medial collateral ligament injuries, meniscus tears, cartilage damage, secondary osteoarthritis).
Contributing Factors / Gear
With the advent of carving skis, it became clear that the increased aggressiveness of the sidecut, combined with stiff boots, leads to more ACL injuries [15]. Tighter turns can be carved, and higher speeds are generated. This demands more strength from the skier and makes controlling the gear more challenging. Due to boot stiffness, the tibia is forced anteriorly when weight shifts backward, placing more stress on the ACL. Furthermore, video analyses revealed that in 100% of the slip-catch cases, the binding failed to release or released too late [15].
Knee Biomechanics in an ACL-Deficient Knee
The primary issue is a combination of anterior knee instability with anterior tibial translation and rotational instability. This alters the entire biomechanics of the knee. The center of rotation in the knee joint shifts medially (inward). This leads to increased stress on both collateral ligaments as well as the meniscus horns, which also places more load on the cartilage surfaces. For example, the medial collateral ligament experiences up to 140% more load, while the posterolateral structures must perform up to 400% more work [17]. During gait, this presents as prolonged flexion during the stance phase and increased anterior tibial translation towards the end of stance [17].
Surgery or Conservative Treatment
Following an anterior cruciate ligament injury, you basically have two options – surgical reconstruction of the ACL followed by physiotherapy, or conservative management with physiotherapeutic measures, keeping the option of surgery open if needed.
In Switzerland, the Swiss Medical Board investigated this question (and published a fact sheet [19] on it): After a comprehensive literature review, the panel concluded that both the surgical and conservative approaches can achieve satisfying results – allowing individuals to return to their previous physical activities in most cases. This is supported by studies evaluating outcomes at one, five, and even up to 15 years post-injury. No significant differences were found when comparing conservative treatment to surgical reconstruction [18].
With conservative treatment, if knee instability persists during physical therapy, you can still opt for surgery later without losing valuable time.
In short: "When choosing a treatment plan, the respective advantages and disadvantages (especially the risks involved in surgery) must be carefully weighed; if in doubt, get a second opinion." [19]
Conservative Therapy
The goal of conservative therapy and physiotherapy after an ACL injury is to restore physiological range of motion, stable knee mechanics, and optimal leg alignment. Following an injury, the body responds with specific biological phases (inflammatory phase, proliferative phase, remodeling phase) that a physiotherapist must navigate to ensure the fastest possible healing and restoration of function.
Based on these healing phases, short-, medium-, and long-term milestones are established for both therapists and patients. In the first 1-2 weeks (inflammatory phase), reducing swelling and managing pain through passive measures like lymphatic drainage and gravity-eliminated, gentle joint mobilization are the main therapeutic focus [20].
During the proliferative phase (weeks 3–6), the focus shifts to regaining full mobility, progressive weight-bearing (transitioning from crutches to full weight-bearing), stabilizing the joint, and strengthening muscular deficits in closed kinetic chains. This is achieved through both passive and active exercises [20].
From the 7th week post-injury (remodeling phase), fully restoring lower limb alignment (hip-knee-ankle axis) and rebuilding muscle through progressive strength training in the gym are key. The ultimate goal is pain-free function in daily life and a successful back-to-sport transition [20].
If you need us, we are here to support you!
Your BodyLab Team – Your Specialists in Recovery and Injury Rehabilitation
Osteopathy and Physiotherapy | Rehabilitation and Training
Zurich Altstetten
References
[1] Sporting Activity and Sports Interests of the Swiss Population.
Lamprecht, M., Fischer, A. & Stamm, H.P.
Sport Schweiz 2014: Sportaktivität und Sportinteresse der Schweizer Bevölkerung. Magglingen: Bundesamt für Sport BASPO.
[2] Injuries by Sport and Age, Ø 2010–2014
[3] Injury Location in UVG Underwriters by Sport (per 100 injured), Ø 2008–2012
Woods C, Hawkins R, Hulse M, Hodson A.
Br J Sports Med. 2002;36(6):436-441. doi:10.1136/bjsm.36.6.436.
[5] The FIFA 11+ injury prevention program for soccer players: a systematic review.
Sadigursky D, Braid JA, De Lira DNL, Machado BAB, Carneiro RJF, Colavolpe PO.
BMC Sports Sci Med Rehabil. 2017;9:18. doi:10.1186/s13102-017-0083-z.
Volpi P, Bisciotti GN, Chamari K, Cena E, Carimati G, Bragazzi NL.
Muscles Ligaments Tendons J. 2016;6(4):480-485. doi:10.11138/mltj/2016.6.4.480.
[7] Soccer-related injuries treated in emergency departments: 1990-2014.
Smith NA, Chounthirath T, Xiang H.
Pediatrics. 2016;138(4). doi:10.1542/peds.2016-0346.
Leininger RE, Knox CL, Comstock RD.
Am J Sports Med. 2007;35(2):288-293. doi:10.1177/0363546506294060
[9] Childhood soccer injuries treated in U.S. emergency departments.
Adams AL, Schiff MA.
Acad Emerg Med. 2006;13(5):571-574. doi:10.1197/j.aem.2005.12.015.
Woods C, Hawkins R, Hulse M, Hodson A.
Br J Sports Med. 2002;36(6):436-441. doi:10.1136/bjsm.36.6.436
[11] Severe injuries in football players. Influencing factors.
Chomiak J, Junge A, Peterson L, Dvorak J.
Am J Sports Med. 2000;28(5 Suppl):S58-68. doi:10.1177/28.suppl_5.s-58.
[12] Anterior cruciate ligament injury in elite football: a prospective three-cohort study.
Waldén M, Hägglund M, Magnusson H, Ekstrand J.
Knee Surg Sports Traumatol Arthrosc. 2011;19(1):11-19. doi:10.1007/s00167-010-1170-9.
Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M.
Br J Sports Med. 2015;49(22):1452-1460. doi:10.1136/bjsports-2014-094573.
Grassi A, Smiley SP, Roberti di Sarsina T, et al.
Eur J Orthop Surg Traumatol. 2017;27(7):967-981. doi:10.1007/s00590-017-1905-0.
BereT, FlørenesTW, KrosshaugT, et al.
Am J Sports Med. 2011;39:1421–1429
Ruedl G, Webhofer M, Linortner I, et al.
Int J Sports Med. 2011; 32 (10):801-6.
[17] Riss des vorderen Kreuzbandes. Biomechanische Auswirkungen auf das Kniegelenk
PD Dr. M. Herbort, Prof. Dr. C. Fink:
in: Arthroskopie (01/2015)
[18] Review Technical Report «Rupture of the ACL: surgical or conservative treatment?»
[19] Fact Sheet Anterior Cruciate Ligament Rupture: surgical or conservative treatment?
[20] ACL Rupture Therapy, AGA Knee Ligament Committee
Cover Image Credits

Kari Stammen, Human Knee Anatomy, designated as public domain, details on Wikimedia Commons



{kind=link}