
Acute Supination Injury - Ligament Injuries of the Foot
January 6, 2020
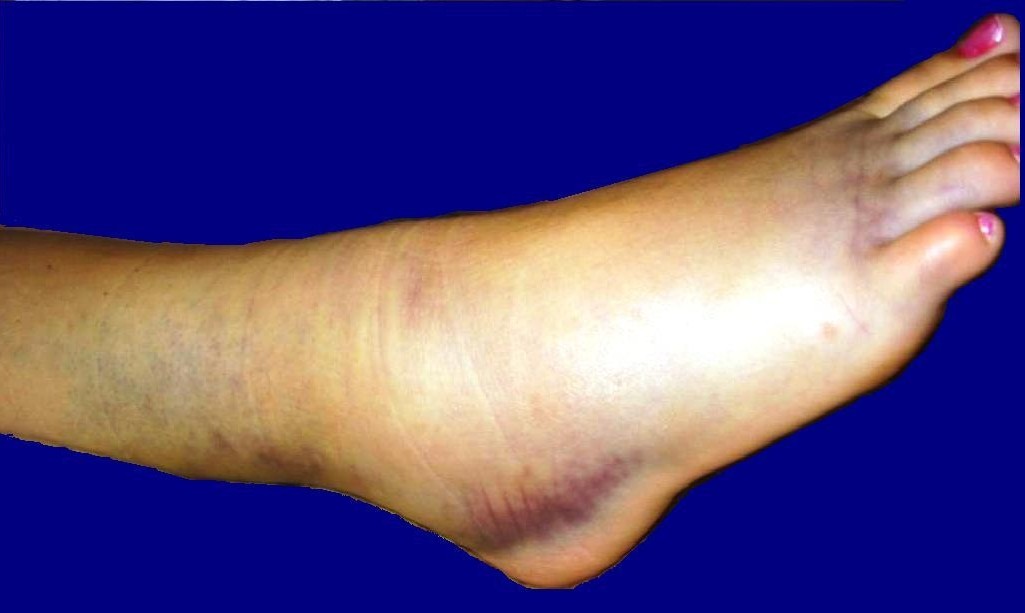
Supination trauma, sprain, ligament injuries or tears of the foot
Ligament injuries of the ankle joint (inversion trauma, ankle sprain, ligament tears) are very common and often occur in everyday life due to a simple misstep or, even more so, during various recreational and sports activities (see accident statistics bfu): An ankle injury is one of the most frequent musculoskeletal injuries to the human musculoskeletal system worldwide.

Boldie, Sprained foot, marked public domain, details on Wikimedia Commons
Despite this, we at BodyLab Osteopathy and Physiotherapy, Rehabilitation and Training in Zurich see different approaches and medical provisions depending on the hospital or doctor: From casts and braces with or without crutches, to tapes or even no immobilizing support at all, with purely physiotherapeutic referrals - especially with sports doctors...
Due to the high number of injuries, various scientific publications and studies deal with this topic. And we at BodyLab have done some research in the literature.
As mentioned in our blog Cruciate Ligament Injuries, different countries have their own committees/medical boards that develop and issue guidelines for such frequently occurring injuries based on the current state of science. Guidelines are protocols that should help the therapist assess whether the healing process of an injury is proceeding normally or not, and recommend adequate therapy and treatment interventions. They provide framework information, serving as a reference.
We find the Dutch "KNGF-Guideline for physical therapy in patients with acute ankle sprain" an important and good paper: because in Holland, patients can go directly to a physiotherapist (without a doctor’s referral), whereby a physiotherapist must know what to do and when! He must be able to rely on and master his differential diagnostics.
Anatomy and function of foot ligaments - Capsule
The ankle joint serves as the connection and thus the transmission of force from the body/lower leg to the foot/ground. It consists of 2 joint parts - the upper ankle joint, formed by the connection of the fibula and tibia (ankle) with the talus, and the lower ankle joint where the talus meets the calcaneus.
The greatest part of stability in the ankle joint is achieved by the arrangement of the bones and by the formation of capsules by many ligaments. The muscles around the ankle originate in the lower leg and are rerouted, except for the Achilles tendon, via retinacula (band structures) or bone notches. Thus, the muscles do not attach directly to the ankle.
Medial and lateral, the joint is stabilized by ligaments. On the medial side, the broad deltoid ligament fan-shaped stretches from the inner ankle to the talus as well as the navicular (tarsal bones) and the calcaneus (heel). Anatomically, the deltoid ligament is divided into 4 parts. The main task of the deltoid ligament is the stabilization against pronation (valgus) and inhibition of eversion. It is one of the strongest ligaments in the body.

Henry Vandyke Carter creator QS:P170,Q955620 Henry Gray creator QS:P170,Q40319, Gray354, marked public domain, details on Wikimedia Commons
On the outside, 3 different bands form the outer ligament – the calcaneofibular ligament and the anterior and posterior talofibular ligaments. They each stretch from the outer ankle to the calcaneus or parts of the talus.
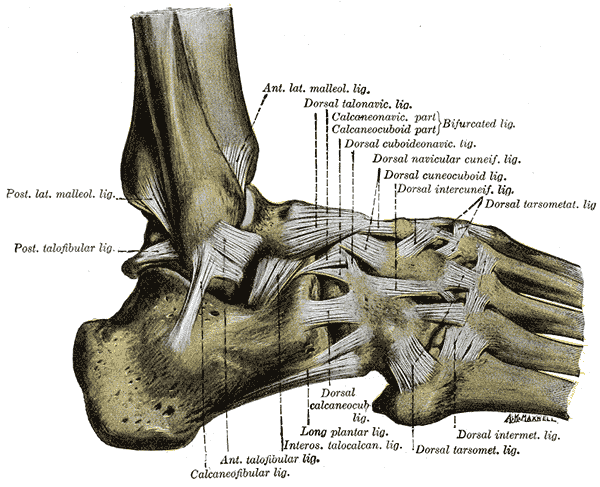
Henry Vandyke Carter creator QS:P170,Q955620 Henry Gray creator QS:P170,Q40319, Gray355, marked public domain, details on Wikimedia Commons
Based on the structural differences of the inner and outer ligaments (width and arrangement), it is obvious that the inner side of the ankle is stabilized much more strongly by passive structures. You can also feel that the foot can be moved further inward than outward.
If the "weaker" outer ligaments are overstretched due to a misstep and inward rolling of the foot, it can easily lead to overstretching of these outer ligaments or even ligament tears.
Injuries and Mechanisms
By treading and rolling inward of the foot, excessive foot movement occurs, which mostly (and first) affects the anterior talofibular ligament. Depending on the severity and force, this band can be overstretched or even torn. Further capsule injuries can occur (since the ligaments are mostly fused with the capsule), further ligament tears of the foot (e.g., bifurcate ligament) or even syndesmosis injuries (connection between tibia and fibula) can occur. Additionally, bone avulsions or fractures may develop.
Due to the rectangular anatomical shape of the talus, impression injuries of the cartilage in the joint fork of the tibia-fibula in the upper ankle joint often occur with bone bruises in the bone. Too excessive tilt of the talus results in high, punctual stress in the upper ankle, causing the patient to experience discomfort and pain on the inside of the joint.
Screening Process
The goal is to identify the problem and the injured structures, as well as to recognize red flags (severe injuries like fractures). Do the symptoms match known clinical signs of a sprained ankle?
Is it an acute sprain from an accident? Or is the problem in a chronic or functional instability? To detect or rule out a fracture after an acute accident, the Ottawa Ankle Rules are helpful. These have almost 100% sensitivity (The definition of a diagnostic test's sensitivity states how many patients with a disease are actually detected by the test), but only moderate (25-50%) specificity (provides information about the proportion of healthy individuals where no disease was diagnosed).
The Ottawa Ankle Rules state:
Can the patient not walk four steps immediately after the injury, or
does he have increased local bone tenderness at the back edges or tips of the malleoli (ankles) at 4 palpation points, or
does he have increased bone tenderness in the area of the navicular or base of the fifth metatarsal
then seeing a doctor with an X-ray is indicated.
Diagnostic Process
The goal of the physiotherapeutic examination and diagnosis is to determine, based on medical and other information, whether physiotherapy can affect and alter the triggering and inhibiting factors that led to the patient’s medical health problem, and can be confirmed by the physiotherapist.
The diagnostic process should result in a physiotherapeutic diagnosis!
The therapist examines and determines the current status and severity of the injury of the capsule-ligament apparatus in relation to the patient’s history and examination. The functional examination includes active tests (active mobility, can weight be placed on the foot), as well as passive and palpatory tests. With these, it should be evaluated differentially which structures are injured (muscle, tendon, cartilage, or capsule-ligament apparatus).
Then it should also be clear to the therapist in which healing phase the tissue is and whether a normal or abnormal healing process is taking place. This allows for prognosis and provides guidance on physiotherapeutic opportunities.
Therapy
We recommend starting physiotherapeutic measures as soon as possible (within 5 days to a week).
The therapy varies according to the current state and condition (healing phase) of the tissue, as well as the patient's symptoms.
In the acute phase (0-3 days after accident), pain-relieving and anti-swelling techniques are indicated. Depending on the pain, partial weight-bearing and elevating the injured foot during this time makes sense! Also, a compression bandage for significant swelling can be considered in this initial stage. Still, the foot and toes should be moved as much as possible without pain.
A very important part of all treatments is patient education and information!
Depending on the severity and healing state, the following steps should focus on gradually resuming functionality and activity depending on the pain level. Start with functional exercises aimed at achieving normal range of motion and promoting foot stability and coordination, as well as achieving normal walking.
Over time, exercises are added to improve foot strength and proprioception.
As explained in our blog on healing, there is no faster healing than optimal healing! At BodyLab, we have the knowledge to optimally support and accompany you as a patient with injuries to the musculoskeletal system. To alleviate your pain and to recognize or prevent delays and complications (such as infections, later deficits) as early as possible. For an optimal, quickest, and best result.
If you need us, we are here for you!
Your BodyLab Team - your specialists after physical injuries
Osteopathy and Physiotherapy | Rehabilitation and Training
Zurich Altstetten
References / Guidelines
KNGF-Guideline for Physical Therapy in patients with acute ankle sprain
Supplement to the Dutch Journal of Physical Therapy, Volume 116 / Issue 5 / 2006
KNGF-Flowchart for Physical Therapy in patients with acute ankle sprain / functional instability
Title image credit
Harrygouvas, ANKLE SPRAIN 02b, CC BY-SA 3.0
Harrygouvas


