
Shoulder Impingement - Subacromial Impingement Syndrome
February 11, 2020
The movements of the shoulder girdle involve 5 different joints—the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, the subacromial space, and the scapulothoracic glide space. Due to this anatomical structure, the shoulder girdle exhibits significant mobility, but it is also more prone to various injuries and shoulder pain. To ensure optimal biomechanical movement, the thoracic spine must be freely movable in addition to the mechanics of the 5 shoulder joints.
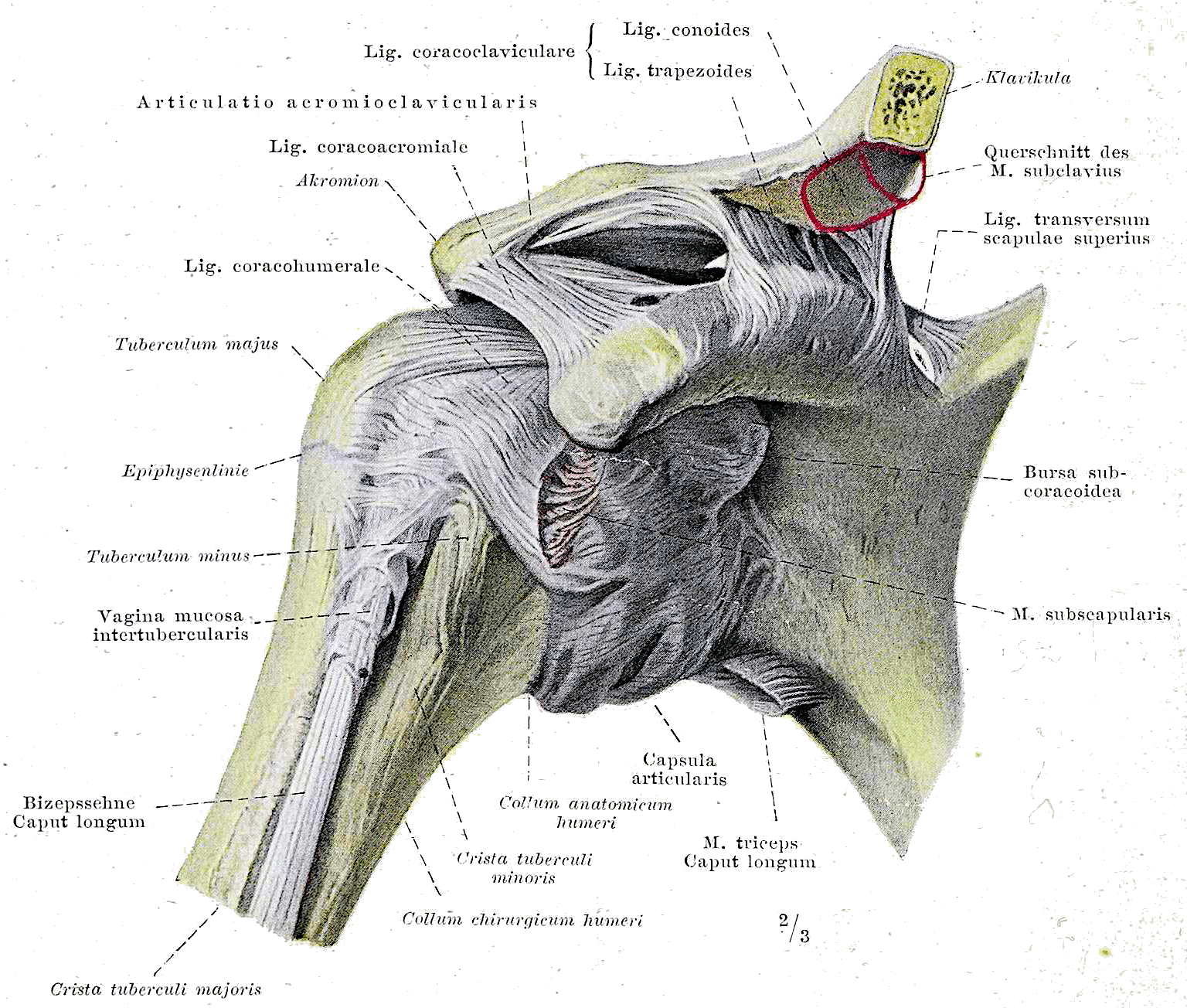
Braus, Hermann, Braus 1921 148, marked as public domain, details on Wikimedia Commons
The anatomical structure of the shoulder joint
The glenohumeral joint (commonly known as the shoulder joint) consists of the humeral head of the upper arm and the glenoid cavity (socket) on the scapula. As a typical ball-and-socket joint, the glenohumeral joint is crucial for the extensive mobility of the shoulder girdle.
The joint surface of the humeral head is three to four times larger than the joint surface of the glenoid cavity, contributing to the high mobility of the shoulder at the expense of stability. The fibrocartilaginous labrum glenoidale (joint lip) at the socket edge, along with the entire capsular-ligamentous apparatus, serves to compensate for this incongruity and improve the stability of the shoulder joint. However, stability is primarily maintained by strong shoulder muscles.
The acromion (shoulder roof) and the clavicle (collarbone) form the acromioclavicular joint. When the arm is elevated above shoulder height, the clavicle rotates along its axis. Through ligaments (acromioclavicular, coracoacromial, and coracoclavicular ligaments), the acromioclavicular joint is held in position during the longitudinal and craniocaudal rotational movements of the clavicle.
The same applies to the sternoclavicular joint, formed by the clavicle and the sternum (breastbone), at the other end of the clavicle. The sternoclavicular joint also includes the articular disc (similar to a intervertebral disc) to balance the incongruity of the joint surfaces of the clavicle and sternum.
After a prolonged immobilization of the arm, adhesions can occur in the capsular-ligamentous apparatus—affecting the ligaments of the acromioclavicular joint, the sternoclavicular joint, and the glenohumeral joint. This leads to restrictions in mobility and biomechanical movement. In the worst case, adhesive or shrinkage of the capsule over time can lead to complications resulting in a frozen shoulder with significant movement restrictions.
The scapulothoracic glide space and the subacromial space are not true joints, but they play a very important role in the biomechanics of the shoulder. The scapulothoracic glide space describes the movement of the scapula on the thorax. Between these, the muscles subscapularis and serratus anterior lie. In shoulder problems, it often becomes apparent that the scapula cannot be sufficiently fixed on the thorax, causing it to move along prematurely during shoulder movements.
The subacromial space is the area between the acromion and the humeral head and consists of two bursae between the acromion and the rotator cuff. Here, the rotator cuff, consisting of the muscles infraspinatus, supraspinatus, subscapularis, and teres minor, plays a central role. The rotator cuff is primarily responsible for centering the humeral head in the glenoid cavity. If any of these muscles are too weak, overloaded after injury, or overstrained due to repetitive movements, the centering and thus the biomechanical process in the shoulder is not ensured. Calcifications or thickenings of the supraspinatus tendon, which runs through the subacromial space, can lead to similar issues.
The musculus supraspinatus runs beneath the acromion from the fossa supraspinata on the scapula to the humeral head. If the function of the supraspinatus is impaired, it leads to dysfunction in the initial phase of arm abduction. More importantly, due to the external rotation function of the supraspinatus, centering the humeral head dorsally in the glenoid cavity is crucial. Without this centering, lateral arm lifting results in subacromial space constriction—the humeral head glides too quickly cranially, and the greater tubercle on the humeral head fails to rotate dorsally in time, striking the acromion and pinching the structures in the subacromial space. During any overhead arm movement, this mechanism irritates the supraspinatus tendon, often leading to inflammation of the bursae and the corresponding joint capsule showing inflammatory signs. The already narrow subacromial space becomes further constrained by the swelling, understandably causing additional problems and pain. This condition is referred to as shoulder impingement or subacromial impingement syndrome.
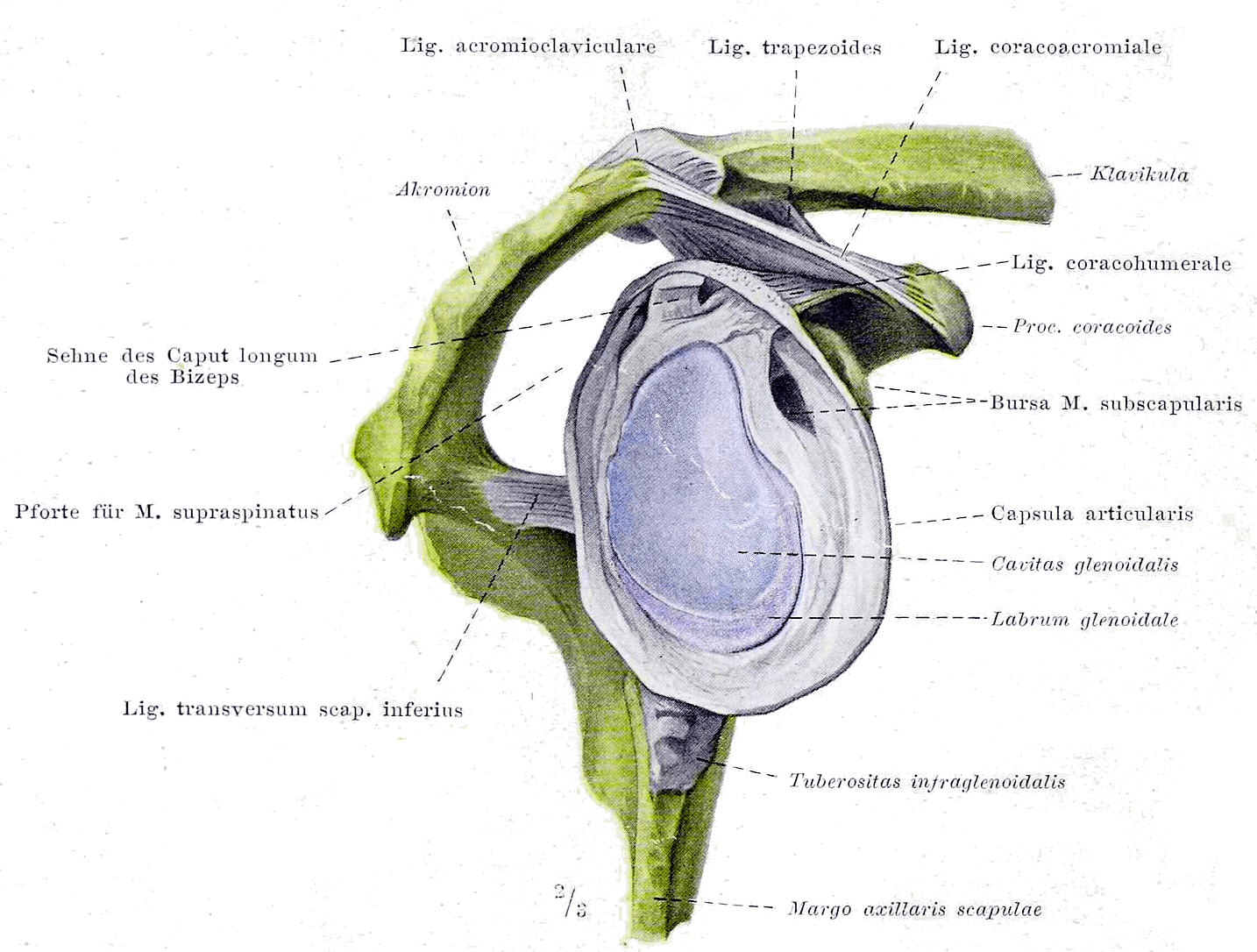
Braus, Hermann, Braus 1921 147, marked as public domain, details on Wikimedia Commons
Treatment of Subacromial Impingement Syndrome – to decompress or not?
Subacromial decompression (acromioplasty) is a widely used minimally invasive surgery for shoulder impingement syndrome.
The surgery typically lasts about an hour and is performed under general anesthesia. Small skin incisions (usually 3 of about 2 sutures each) allow the introduction of surgical instruments. During the operation, bone on the underside of the acromion is removed, and the bursa may be excised (bursectomy), creating more space in the subacromial glide area to resolve the narrowing. Additionally, the surgeon repairs any tendon damage as necessary.
As discussed in the article Meniscus injuries in arthritic knee: surgery yes or no?, at BodyLab | Osteopathy and Physiotherapy | Rehabilitation and Training | Zurich, we always question what added value a surgery provides for the patient.
A recent review [1] examined 9 studies with a total of 1014 patients aged 43 to 57 years regarding pain, joint function, Global Perceived Effect (GPE), and quality of life evaluated 6 and 12 months postoperatively. The control groups consisted of active physiotherapy (6 studies), placebo surgery (2 studies), laser treatments (1 study), a standalone bursectomy (1 study), and waiting (1 study).
The following results were found for the respective evaluation factors:
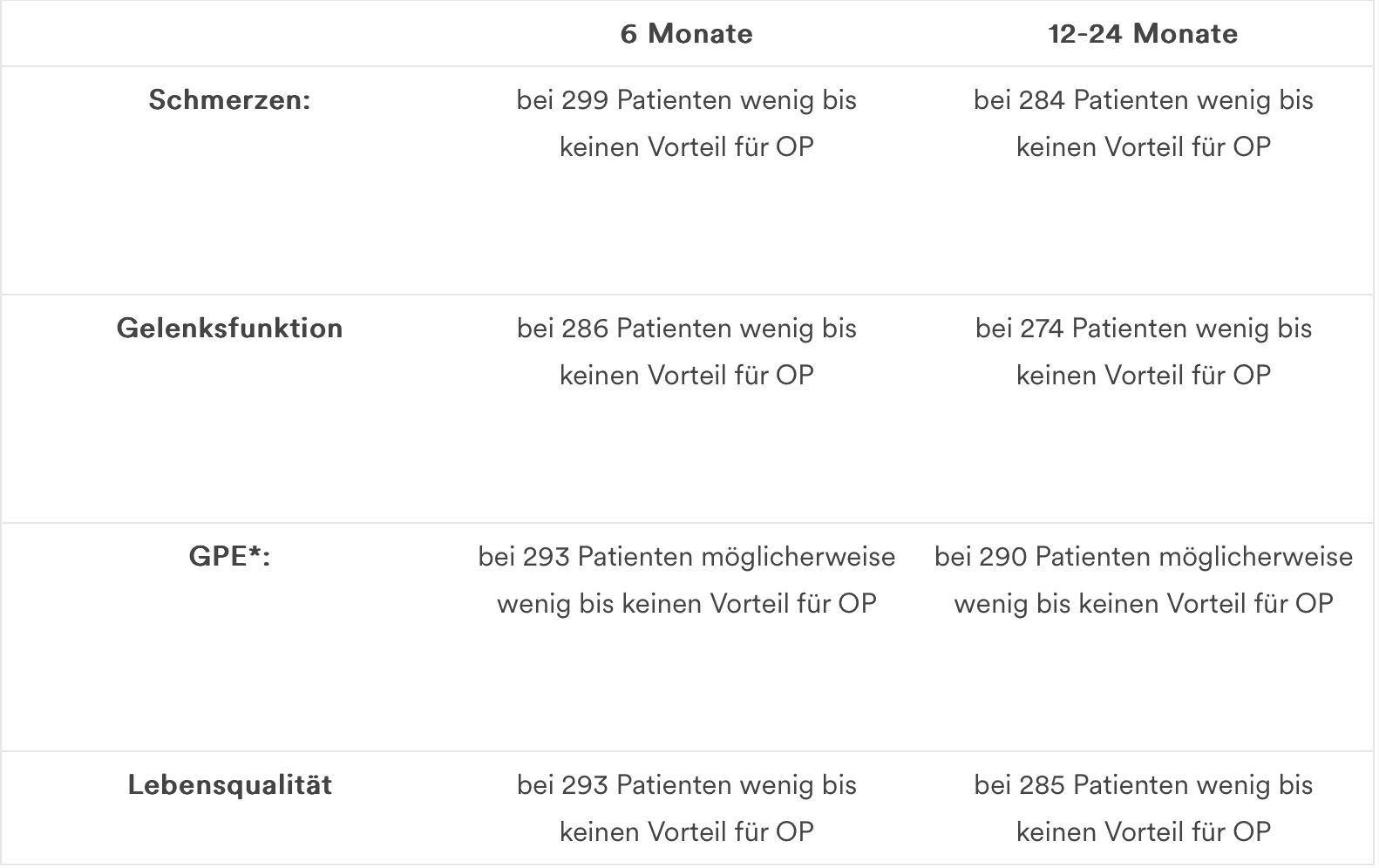
*moderate evidence due to imprecise measures
Previously, acromioplasty was known to be a common standard procedure for subacromial impingement. Clear advantages over conservative therapy (exercise/training, physiotherapy) have not been consistently demonstrated by studies.
Newly, there appears to be no significant difference, especially when comparing acromioplasty with placebo surgery in terms of pain, joint function, and quality of life, each 6 to 12-24 months postoperatively. Comparing with active physiotherapy, there is a small but insignificant difference regarding pain relief (moderate evidence) and less persistent restrictions in mobility/joint function (low evidence).
In conclusion, subacromial decompression as a standard solution for shoulder impingement should be reconsidered by doctors, healthcare providers, hospitals, and insurers (health insurance companies).
As physiotherapists and osteopaths, we recommend carefully weighing the pros and cons of surgery and, whenever possible, starting with a conservative approach first.
Conservative treatment options for shoulder impingement
The goal of conservative treatment in physiotherapy or osteopathy is to restore the biomechanics of the shoulder girdle in subacromial or shoulder impingement syndrome, as well as stabilize and strengthen the shoulder. Particularly in osteopathy, through manual mobilization and manipulation techniques, as well as fascial and soft tissue techniques, the joints and muscles of the thoracic spine and shoulder girdle are loosened to alleviate any pain and improve mobility.
In the physiotherapeutic area, following anti-inflammatory measures, the focus is on activating the rotator cuff for stabilizing and centering the glenohumeral joint. Subsequently, through active exercises, the scapulothoracic rhythm is learned, as well as the active fixation of the scapula on the thorax.
If you need us, we are here for you!
Your BodyLab Team – Your Shoulder Pain Specialists
Osteopathy and Physiotherapy | Rehabilitation and Training
Zurich Altstetten
References
Lähdeoja T, Karjalainen T, Jokihaara J, et al
British Journal of Sports Medicine Published Online First: 15 January 2019. doi: 10.1136/bjsports-2018-100486
Title Image Credit

Henry Vandyke Carter creator QS:P170,Q955620 Henry Gray author QS:P170,Q40319, Gray326, marked as public domain, details on Wikimedia Commons


