
Menisci
July 16, 2018
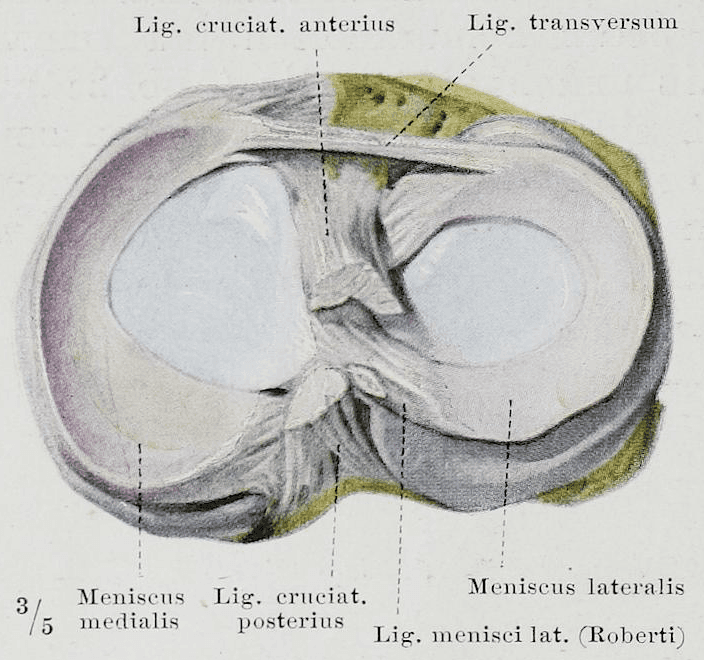
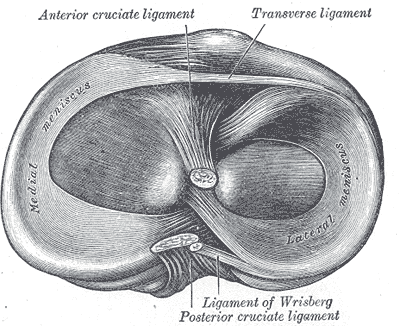
Each of our knee joints contains two menisci. These are two large, fibrocartilaginous wedges. They differ slightly in shape, are fully situated within the joint, and are enclosed by the joint capsule. The outer (lateral) meniscus has a more rounded O-shape, while the inner meniscus exhibits a more crescent-like C-shape. Both menisci are divided into a posterior and an anterior horn.
Tasks and Functions
The task of the menisci is to compensate for the considerable difference between the upper and lower leg of the knee joint and to reduce joint incongruence. This increases the stability of the knee joint while simultaneously reducing the load on the hyaline joint cartilage surfaces of these bones.

Henry Vandyke Carter creator QS:P170,Q955620 derivative work: Hellerhoff Henry Graycreator QS:P170,Q40319 , Gray348-2, marked as public domain, details on Wikimedia Commons
Structure
The menisci are also a connective tissue structure made up of cells and matrix. Physiologically, they are comparable to joint cartilage (also see our blog Joint Cartilage). Menisci consist of about 75% water.
Both menisci are thickest in the outer area and become thinner towards their center. The outer thicker area also contains most of the cells and is most intensively innervated and vascularized there.
Braus, Hermann, Braus 1921 284, marked as public domain, details on Wikimedia Commons
The alignment and orientation of the fibers vary greatly in different areas depending on the load and requirement.
As the menisci are only supplied with blood and nerve endings in the outer thicker areas, good quality synovial fluid is crucial for their supply (the synovial fluid is produced by the joint capsule). To promote and support diffusion and osmosis processes, they need a regular alternation between loading and unloading to maintain their structure and function.
Henry Vandyke Carter Henry Gray, Gray348-de, marked as public domain, details on Wikimedia Commons
The menisci are fused with the joint capsule in the outer area, but the inner medial meniscus is much firmer (due to its additional connection with the inner ligament of the knee, which is more strongly connected to the joint capsule and the medial meniscus on the inside than on the outside). This gives the outer lateral meniscus more mobility than the inner medial one - due to this reduced mobility of the medial meniscus, it is correspondingly more prone to traumatic injuries.
Degeneration and Trauma
The most common causes of problems are age-related or immobilization-induced degenerative changes, as well as traumatic injuries.
If the joint does not move, degenerative changes occur very rapidly.
During immobilization, a high loss of water and ground substance very quickly occurs, which means that the collagen network is no longer tensioned (just like joint cartilage), thus significantly reducing the load capacity of the cartilage and menisci.
Due to the increased deformability of the menisci, the load on the fiber network increases. At the same time, the mobility of the menisci concerning the joint cartilage surface decreases.
In principle, all movements in the knee joint with a high degree of movement and/or speed can cause injury to the menisci. Most often, they are traumas that occur through combination movements (bending, buckling, and external rotation). As explained above, because the inner medial meniscus has less mobility, it is more prone to injuries and more frequently affected by traumatic injuries. Not infrequently, the aforementioned combination movement can result in the involvement of the medial collateral ligament of the Lig. collaterale mediale (inner ligament) and the anterior cruciate ligament (so-called unhappy triad).
Training
Just as with joint cartilage, training and thus micellar alignment improve the menisci's tensile strength. Furthermore, through reversible hypertrophy (more cartilage cells are formed), the incongruence is reduced by enlarging the contact surfaces. This improves pressure elasticity and shock absorption in the knee joint.
Training and exercises not only improve the adaptability of cartilage tissue: strengthening the skeletal muscles and improving coordination relieve the knee joint during movements, especially under higher loads, thereby protecting the tissue and the body.
Therapy
To ensure optimal wound healing and regeneration of injured tissue, regular physiological loading of the same is required. Only in this way can the body rebuild new, functional, and loadable tissue. Without corresponding physiological stimuli, decreased replacement or scar tissue is formed with reduced quality.
For knee injuries, patients should therefore move and load the knee in a reduced form if possible.
In the physiotherapy and osteopathy at BodyLab, we understand the anatomical and physiological conditions. We know which therapeutic and training options exist in the event of injuries or complaints/problems and are happy to advise and instruct you in this regard.
If active loading is not yet (after operations or injuries) or no longer possible, we can use passive joint techniques, partially under compression or traction, to improve the quality and function of the menisci and the whole joint as a functional unit, which reduces pain and complaints.
Once again, it is true: Life means movement!
If you need us, we are happy to be there for you!
Your BodyLab Team - Your Connective Tissue Specialists
Osteopathy and Physiotherapy | Rehabilitation and Training
Zurich Altstetten
Further information on cartilage tissue can also be found in our blog on our homepage under Joint Cartilage.
Learn more about our intervertebral disc - structure & function in another blog.
Cover Image Credit
Henry Vandyke Carter Henry Gray, Gray349, marked as public domain, details on Wikimedia Commons


